
One of the most prevalent foot disorders is plantar fasciitis, which affects 11–15% of adults at some point in their lives. Plantar fasciitis may exhibit both inflammatory and degenerative features, according to histopathology. This can be ascribed to bad work habits, over loading, and overuse. When we talk about an unparalleled insight into plantar fasciitis we mean a comprehensive understanding about the physiology and real world case study that can help the readers gain knowledge about the condition.
Table of Contents
ToggleWhat really happens in Plantar Fasciitis?
A thick slash of fibrous tissue present at the sole is known as plantar fascia. It extends to the middle, medial and lateral aspects of the foot originating from the medial tubercle of calcaneus and inserting at the metatarsal heads. The arch of the foot is stabilized and maintained by the fascia. When this fibrous tissue gets inflamed due to overuse, a condition known as plantar fasciitis eventuates. It is more common in middle aged individuals and athletes.
Symptoms
- Sharp and stabbing pain as soon as you wake up or when you stand after prolonged periods of sitting
- Worsening pain after prolonged standing that may radiate to the tarsals or towards the calf depending on the tension
- Tenderness on touch
Chronic Changes
- When inflammation persists, the plantar fascia tissue may experience degenerative changes, such as thickening, collagen degradation, and tiny tears.
- Research has shown that up to 80% of individuals may still have symptoms a year following diagnosis, and many nevertheless experience some discomfort in their heels.
- Patients with chronic pain & inflammation at the fascia may begin to modify their posture as well as gait pattern and prefer limping over normal stance. This increases complications.
- Prolonged inflammation can lead to inability to bear weight on that foot causing functional limitation during various activities.
- One of the major changes that might occur due to chronic inflammation of the fascia is the formation of heel spurs. A heel spur is known as the osteophytic growth that forms at the bottom of the calcaneal bone, an area where the fascia attaches to the calcaneum.
Learning through a Case Study
A 54 year old female nurse presented to the Rehab OPD with the complaint of heel discomfort as soon as she wakes up in the morning. The pain was described as sharp, shooting and was given a rating of 10 on Numeric Pain Rating Scale. She claimed that after a short while of walking, the pain gradually went away, but it returned and got worse when she stood and walked for extended periods of time during her duty hours, which had a big impact on her ability to execute her job. She also reported difficulty in plantar flexion along with flexion of the toes when walking.
The patient further revealed that she had a history of fall two weeks prior from a ladder whilst she was renovating her house. She landed on a coffee table during the fall and was struck hard in the lower back. There were no reports of lower limb numbness, tingling, radiating pain along the limb, or direct heel injuries.
Clinical Examination to rule out the Differential Diagnosis
Upon examination it was divulged that the patient experienced:
- Localized tenderness at the medial calcaneal tubercle when gentle pressure was applied on her bony prominence.
- No sensory deficits were observed such as numbness, tingling or loss of sensation of touch at the lower limb. The reflexes were intact.
- The neurodynamic tests such as Straight Leg Raise Test & Slump Test were negative indicating that any nerve root isn’t involved. Read more about it in our previous blog Disc vs Piriformis
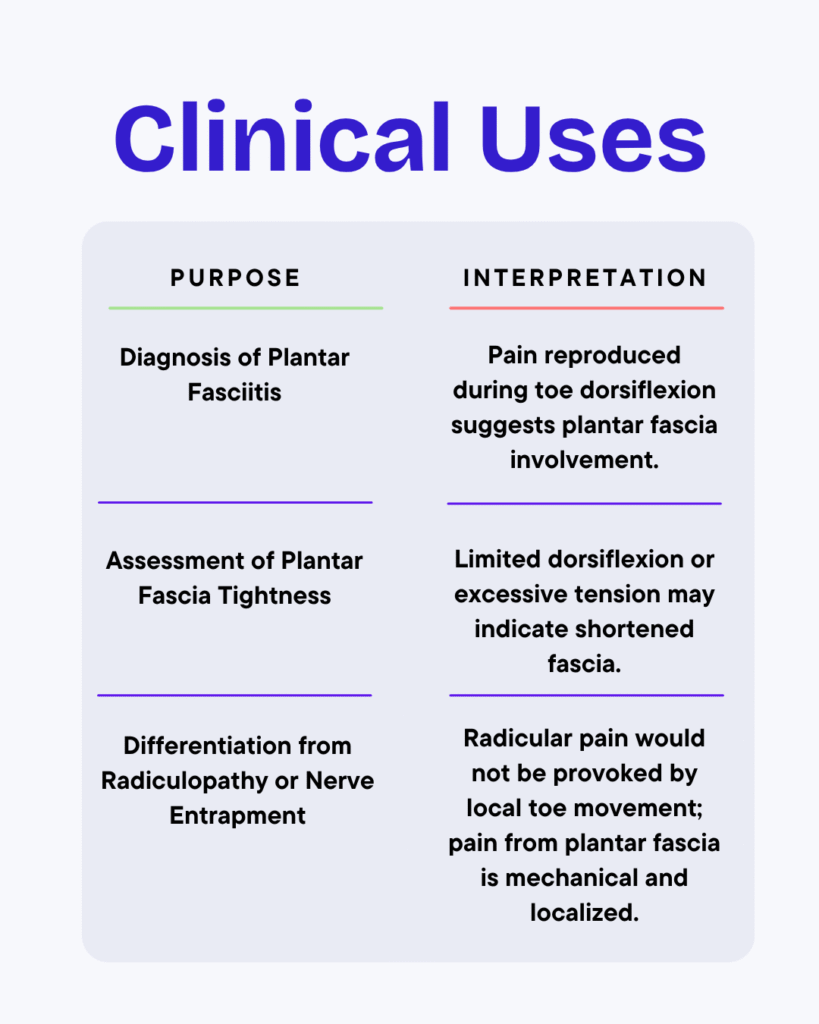
- The pain was provocative on passive dorsiflexion indicating a positive Windlass Test which is the classical finding to prove plantar fasciitis.
Windlass Test or Jack’s Test
A clinical examination test used to test the integrity of the plantar fascia.
- The patient can be tested in weight bearing as well as non weight bearing position.
- Ask the patient to comfortably sit on the chair with both feet straight on the ground.
- Stabilize the ankle in a neutral position and passively dorsiflex the big toe.
- The test is +ve if the patient reports sharp, shooting pain on the medial calcaneal tubercle or along the path of the plantar fascia.
Diagnosis
A diagnosis of Plantar Fasciitis owing to mechanical strain and overuse was made based on the clinical presentation, which included the absence of neurological symptoms, site specific inflammation & tenderness, and the typical first-step pain in the morning. The patient’s fall probably caused compensatory weight bearing or modified gait mechanics, which over time placed more strain on the plantar fascia and caused inflammation and microtrauma at the calcaneal connection.
To summarize & differentiate this diagnosis from Lumbar Radiculopathy:
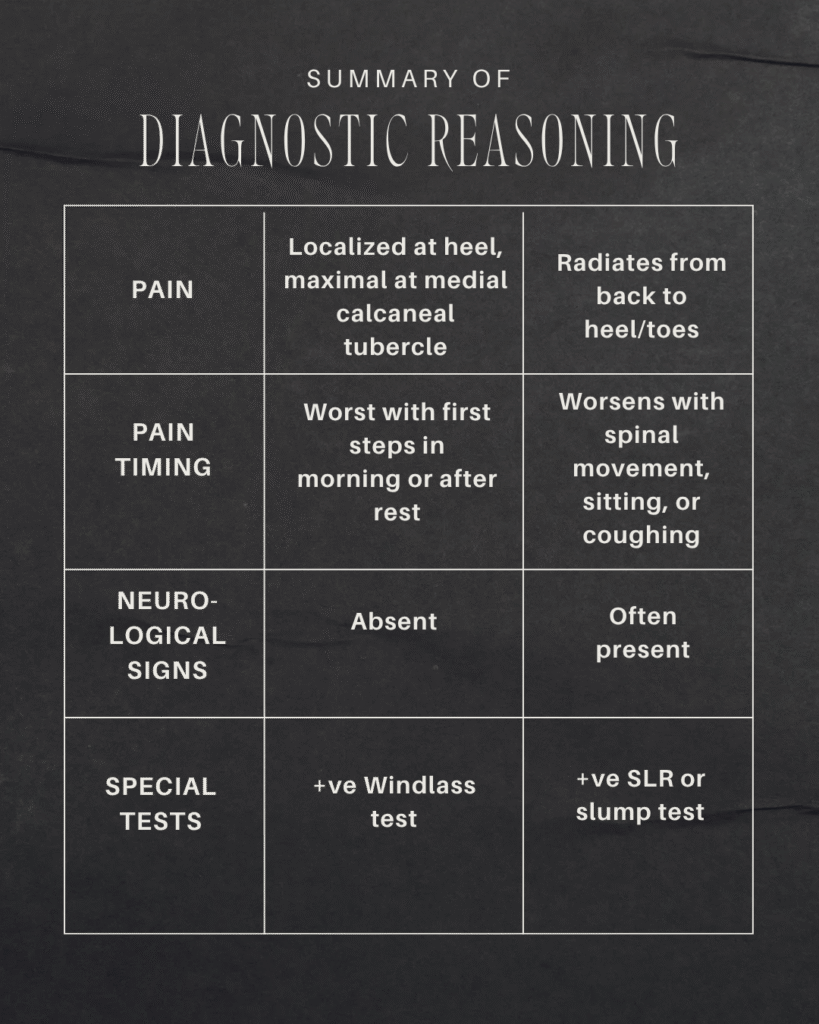
Can you guess which features best represent plantar fasciitis & lumbar radiculopathy? Answer in the comments below.
Common Muscles that are affected due to PF
Triceps Surae - Gastrocnemius & Soleus
- Extrinsic Posterior Leg Muscles
- Functions in the Plantar Flexion of the ankle as well as eccentric dorsiflexion control during walking
- Plantar fasciitis may cause tightness in these muscles increasing tension during gait
Tibialis Posterior
- Extrinsic Deep Posterior Leg Muscle
- Functions as a support to the medial longitudinal arch & helps in inversion & plantar flexion of the foot
- An increased amount of strain on the plantar fascia may cause over pronation of the foot leading to the collapse of the arch
Flexor Digitorum Longus & Flexor Hallucis Longus
- Extrinsic Flexor Muscles of the Toes
- Functions in flexing the toe and helps stabilize it during the push off phase of the gait cycle. These muscles also assist the medial longitudinal arch.
- Can become tight and tender along with the fascia
At this point we’ve addressed what plantar fasciitis is, its symptoms, and the long-term problems that can happen with chronic cases. Along with a detailed case study that shows its clinical appearance, diagnostic rationale, and how it differs from other conditions, we can move on to the next important part: treatment. Now that an unparalleled insight into plantar fasciitis has been laid, let’s examine the therapeutic techniques, physiotherapy treatments, and evidence based management options that can assist plantar fasciitis sufferers in regaining function, minimizing pain, and avoiding recurrence.
Exercises that can help treat Plantar Fasciitis
Arch Roll of Plantar Fascia
- Position the patient comfortably on a chair in a sitting stance and place the tennis ball below the affected foot.
- Roll the ball gently under the arch and heel.
- Continue this for 3 to 5 minutes 2 times per day.
- This will help in the reduction of adhesions and promotes soft tissue mobility.
- To perform accurately watch Ball Rolling Exercise
Calf Stretches
- Position the patient in a way that he is facing the wall, placing his hand on it for support.
- Place the affected heel back and bend the front knee to lean on the wall.
- Bend forward in a way that you feel a stretch on your calf muscles of the affected foot.
- Hold the stretch for 20 to 30 seconds & perform this 2 times per day as per patient’s tolerance.
- This stretch helps release the tension on the Achilles and Fascia.
- How to perform Calf Stretches
Heel Raises
- Ask the patient to stand on any raised edge so the balls of his feet rest on the edge of the surface & heels are off the balance.
- Raise both the legs and then gradually shift to raising only the affected leg.
- Continue to lower your leg with eccentric loading.
- Repeat this exercise 10 to 15 times twice daily or as per patient’s tolerance.
- Loads the Achilles & fascia in a controlled fashion promoting healing & strengthening. Most effective exercise for acute conditions.
- How to perform Heel Raises
Resisted Foot Inversions
- Ask the patient to sit with the affected knee on top of the other in a flexed manner.
- Place the band around the arch and support it on the other end by placing beneath the foot on the ground.
- Invert the foot gradually against the band.
- Repeat 10 to 15 times twice daily or as per tolerance.
- This exercise helps in strengthening the tibialis posterior which is the supporting muscle of the medial longitudinal arch.
- Strengthening of the Tibialis Posterior
Towel Curls
- Place a towel on the floor and ask the patient to place his foot on the towel.
- Instruct the patient to scrunch the towel through his toes.
- Repeat this for 10 to 15 times twice daily or as per tolerance.
- Toe curls help strengthen the intrinsic muscles of the foot such as the flexor digitorum brevis as well as interossei. These muscles support the arch as well & strengthening them improves the overall loading.
- Towel Scrunches for plantar fasciitis
What you should NOT do!
- Avoid walking barefoot especially on rough surfaces
- Do not run or jump excessively
- Avoid prolonged standing or weight bearing positions
- Change your position regularly during work between sitting and standing
- Gradually increase the functional activities as per tolerance
- Do not overstretch the muscles during exercise
- Avoid heat therapy
Quick FAQs
Is Plantar Fasciitis Permanent?
No, plantar fasciitis typically resolves on its own. Most patients heal fully in a few months with the right care, stretching, and supportive footwear. Neglecting the pain, however, may cause it to worsen or result in heel spurs.
How long does it take to recover from PF?
Although recovery times vary, most instances get better after 6–12 weeks of regular physiotherapy. With respect to the severity and the degree of adherence to the treatment plan, chronic cases might take anywhere from three to six months.
Can Plantar Fasciitis reoccur?
Yes, it can recur if preventive measures are not taken, such as avoiding stretches, wearing shoes that don’t provide support, or standing for extended periods of time without taking breaks. Recurrence can be avoided with comfortable footwear and regular foot workouts.
Should I avoid walking in PF?
Avoid abrupt increases in activity, wearing flat or unfriendly footwear, standing for extended periods of time without rest, and going barefoot on hard flooring.
When should I see a Physiotherapist?
See a physiotherapist for a diagnosis and individualized therapy if your heel discomfort persists for longer than two weeks, interferes with your capacity to walk, or gets worse after at home care.
Can Medicines alone treat PF?
No, plantar fasciitis cannot be fully cured by medication alone. The underlying reason, which is typically stiffness, weakness, or excessive strain of the plantar fascia and adjacent muscles, is not addressed by painkillers or anti-inflammatory medications (such as NSAIDs), even though they may momentarily lessen discomfort and swelling.
This article has been written by a Physical Therapist and provides general guidance on physical health & exercise. While it is grounded in professional expertise, it is not a substitute for individualized medical advice. If you are experiencing pain, specific symptoms, or have an underlying medical condition, please book a 1 on 1, 30 minute consultation with our expert physical therapist for a personalized assessment & tailored recommendations.